In the episode, we briefly touched on the role of locking plates in the setting of distal radius fractures. Here, we will expand more on the purpose of locking plates, as well as the technique and indications for their use.
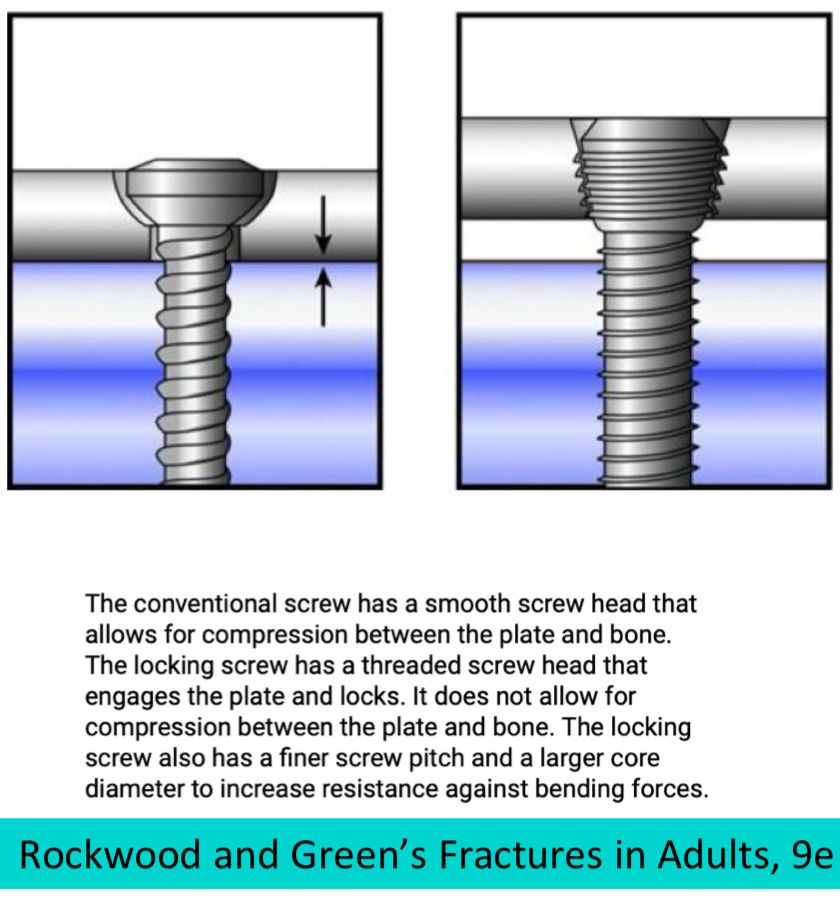
Locked plating is a slightly more sophisticated fixation technique vs. non-locked plating, designed to stabilize fractures in scenarios where traditional plating methods may not suffice due to poor bone quality or complex fracture patterns. The principle of this system revolves around the interaction between locking screws and plates. These screws possess "male" threads that interlock with "female" threads within the plate holes, creating a fixed-angle, stable construct when coupled together.