Episode 4
Clavicle Fractures
Listen to Episode:
Objectives:
After listening to this episode, we hope that you can:
- Identify key physical examination findings indicative of clavicle fractures.
- Summarize the diagnostic process and management strategies for clavicle fractures.
- Gain preliminary insights into surgical techniques for treating clavicle fractures.
- Appreciate the significance of shared decision-making and the application of evidence-based medicine in orthopaedic care.
Show Notes
Episode 4: Clavicle Fractures
Clavicle Anatomy Review
The clavicle, also known as the collarbone, is a crucial bone that connects the arm to the body, playing a pivotal role in the mobility and stability of the upper extremity. Its unique sigmoid shape and its position as a bridge between the axial and appendicular skeleton make it an integral component of the pectoral girdle. Understanding the clavicle's anatomy, including its articulations, ligamentous attachments, and muscular attachments, is fundamental for diagnosing and managing shoulder-related injuries and conditions effectively.
In this section, we will cover essential anatomical features of the clavicle, which are commonly asked about in the operating room.
Articulations and Ligamentous Attachments
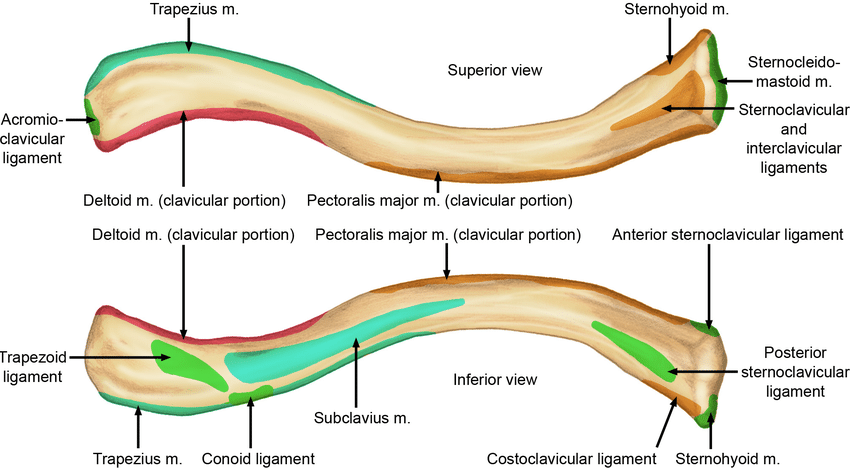
Medial: The clavicle's medial end articulates with the manubrial portion of the sternum at the sternoclavicular (SC) joint. This articulation is fortified by a fibrous capsule and an intra-articular disc, enhancing the joint's stability. The interclavicular ligament spans the medial ends of both clavicles, providing additional support. The costal tuberosity, an inferior feature, is the attachment site for the costoclavicular ligament, supporting the SC joint.
Lateral: Laterally, the clavicle meets the acromion of the scapula at the acromioclavicular (AC) joint. This joint is similarly supported by a fibrous capsule and an intra-articular disc. Key ligaments include the acromioclavicular (AC) ligament, the coracoclavicular (CC) ligament, and the coracoacromial (CA) ligament, which collectively stabilize the AC joint and support shoulder movement. The conoid and trapezoid parts of the CC ligament, which attach inferiorly, provide significant stability between the clavicle and the coracoid process of the scapula.
Image from Harris, Joshua & Griesser, Michael & Jones, Grant. (2012). Acromioclavicular Joint and Clavicle Injuries.
Muscular Attachments
The clavicle serves as a crucial attachment site for various muscles that facilitate the movement and stability of the shoulder:
Medial Two-Thirds: This portion provides attachment for the sternocleidomastoid (SCM) muscle superiorly and the subclavius muscle inferiorly. The anterior surface serves as an attachment site for the pectoralis major, and the posterior surface for the sternohyoid muscle.
Lateral Third: The attachment sites for the deltoid and trapezius muscles are found anteriorly and posteriorly, respectively.
Image from Harris, Joshua & Griesser, Michael & Jones, Grant. (2012). Acromioclavicular Joint and Clavicle Injuries.
Neurovascular Anatomy
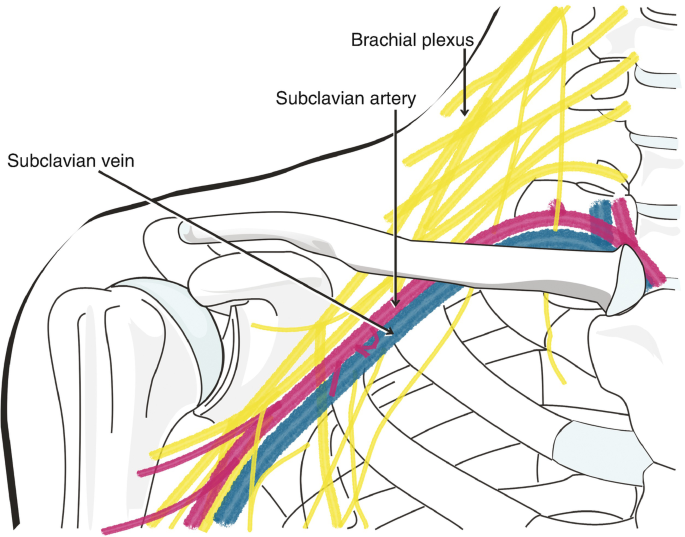
The clavicle is in close proximity to critical vessels for blood supply to the upper extremity, most notably the subclavian artery and vein. The subclavian artery, which passes posterior to the clavicle, provides essential blood flow to the upper limb through the axillary artery. Key branches of the subclavian artery, such as the suprascapular and dorsal scapular arteries, supply blood to the shoulder region and upper back. These vessels are in close proximity to the clavicle and are at risk during operative interventions for clavicular fractures.
The proximity of the brachial plexus also means that neurovascular caution is paramount. The supraclavicular nerves, which branch from the cervical plexus, emerge around the midportion of the clavicle and extend inferiorly and laterally across the upper chest and shoulder area. They are primarily sensory, providing cutaneous innervation to the skin over the upper chest, shoulder, and proximal part of the arm. During surgical procedures to repair clavicle fractures, especially those requiring extensive dissection or the use of hardware for fixation, there is a risk of inadvertently injuring the supraclavicular nerves. Damage to these nerves can lead to sensory deficits in their distribution area, manifesting as numbness or altered sensation over the upper chest and shoulder.
Overall, surgeons must navigate carefully to prevent damage to the neurovascular structures that run adjacent to the clavicle, which could lead to complications such as nerve injury, bleeding, hematoma formation, or ischemia of the upper limb.
Image from Nanda, R., Rangan, A. (2019). Clavicle Fracture. In: Trail, I., Funk, L., Rangan, A., Nixon, M. (eds) Textbook of Shoulder Surgery . Springer, Cham.
Additional Resources