Episode 5
Acute Knee Injuries
Listen to Episode:
Objectives:
After listening to this episode, we hope that you can:
- Describe the acute knee exam that should be performed in an ER or acute setting.
- Understand the anatomy and physiological function of the meniscus, as well as the categories of different meniscus pathologies such as degenerative vs traumatic, radial vs longitudinal, and key patterns such as bucket handle and meniscus tears.
- Identify common mechanisms of injury, and well as the key clinical features that follow.
- Classify meniscal tears and understand what makes a meniscus tear viable for repair or not, and what some corresponding surgical options would be.
Show Notes
Episode 5: Acute Knee Injuries
Acute knee injuries can be deceptively complex. Beyond identifying ligamentous or meniscal pathology, clinicians must remain alert to limb-threatening vascular injuries and associated soft-tissue damage that can significantly alter management and prognosis. This is especially true in cases of suspected knee dislocation or multiligamentous knee injury (MLKI), where vascular compromise may be present even when the joint appears anatomically reduced.
The sections below expand on critical components of the lower extremity vascular examination, including when and how to use Doppler assessment, ankle–brachial index (ABI), and CT angiography. We also review key risk factors for MLKI that should heighten clinical suspicion.
We also delve further into the vascular anatomy of the meniscus, which directly influences healing potential and surgical decision-making in acute knee trauma.
The Lower Extremity Vascular Exam
Why the Vascular Exam Matters
Acute knee injuries—particularly those involving suspected knee dislocation or multiligamentous knee injury (MLKI)—carry a significant risk of popliteal artery injury. Importantly, many knee dislocations spontaneously reduce prior to presentation, meaning the limb may appear anatomically aligned while a limb-threatening vascular injury is still present.
Missed vascular injury can result in ischemia, compartment syndrome, limb loss, or death, making early recognition and investigation critical.
Palpate Distal Pulses
- Assess dorsalis pedis and posterior tibial pulses
- Compare bilaterally
- Document pulse quality
Normal pulses do NOT exclude vascular injury due to collateral circulation.
Assess for Hard Signs of Vascular Injury
Any of the following:
- Absent distal pulses
- Expanding or pulsatile hematoma
- Active hemorrhage
- Signs of ischemia (pain, pallor, paresthesia, paralysis, poikilothermia)
These require immediate vascular surgery consultation.
Use Doppler Ultrasound*
Perform handheld Doppler if pulses are not palpable (if pulses are palpable, can skip). Also, make sure to ompare Doppler signals bilaterally. A Dopplerable pulse is reassuring but not definitive.
Calculate the Ankle–Brachial Index (ABI)
ABI = Ankle systolic pressure / Brachial systolic pressure
- ABI ≥ 0.9 → low likelihood of major vascular injury
- ABI < 0.9 → CT angiography required
- ABI is a key screening test in suspected knee dislocation
Definitive Imaging
CT angiography (CTA) is the gold standard for vascular assessment
This is Indicated for:
- ABI < 0.9
- Absent or asymmetric pulses
- Abnormal Doppler findings
- High clinical suspicion (including high-BMI or high-energy injuries)
Risk Factors for Multi-Ligamentous Knee Injuries
Multiligamentous knee injuries are most commonly associated with high-energy trauma, but may also occur with lower-energy mechanisms in certain populations.
Key risk factors:
High-energy mechanisms
- Motor vehicle collisions
- Motorcycle accidents
- Pedestrian-struck injuries
Concomitant fractures
- Patella
- Tibia
- Femur
Patient factors
- Young, male patients are more frequently affected
- High BMI, which increases axial and rotational forces across the knee, leading to ultra low velocity knee dislocations
Pearl: Patients with high BMI may sustain knee dislocations and MLKIs from low-energy mechanisms, such as simple falls or twisting injuries.
When to Have a High Index of Suspicion?
- Suspected or confirmed knee dislocation
- ≥2 ligament injuries
- Gross knee instability
- Significant swelling or ecchymosis
- Peroneal nerve deficits
- High-energy trauma or high-BMI patients with low-energy mechanisms
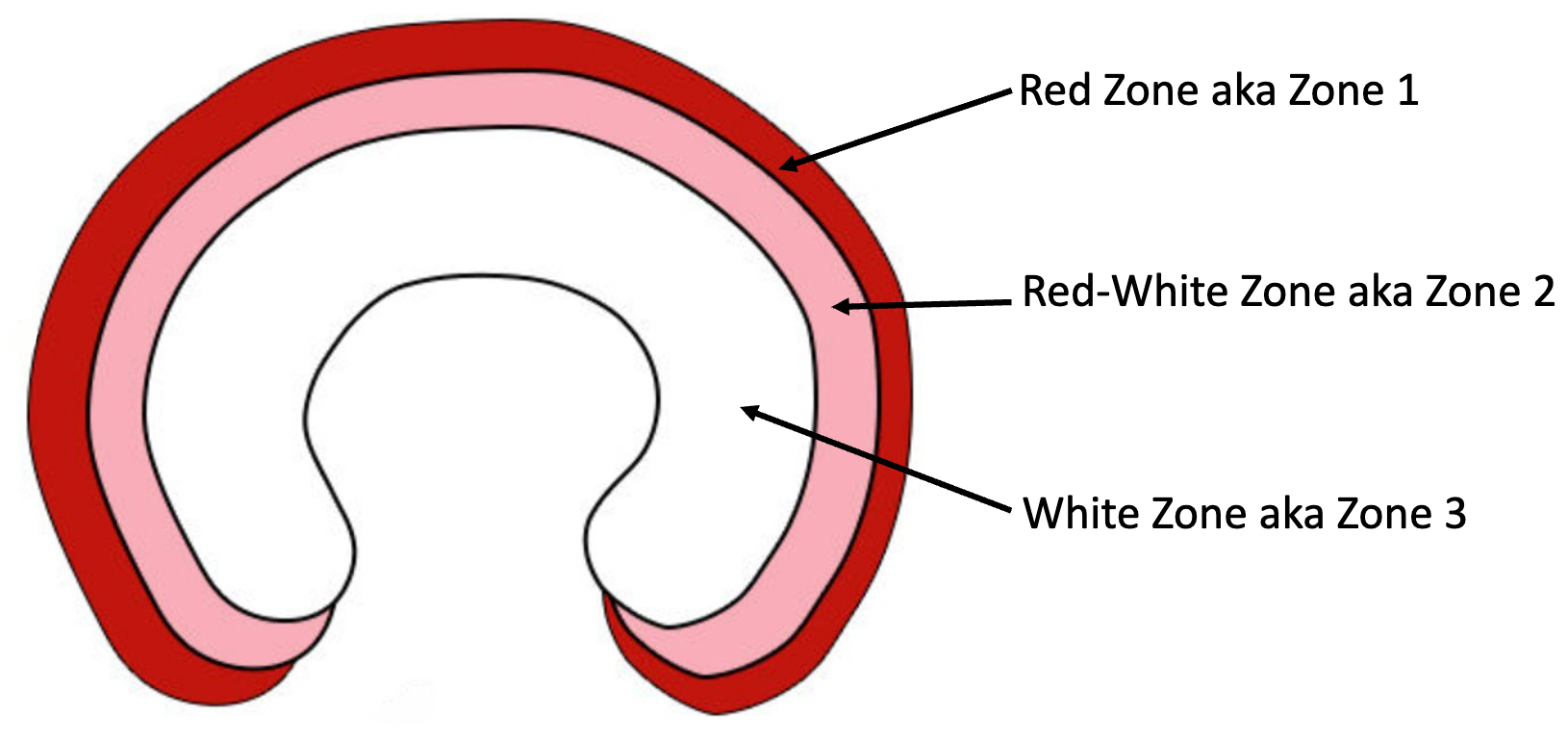
Meniscus Vascular Supply & Zones
The meniscus has a limited blood supply, which is critical for healing after repair.
- The outer one-third of the meniscus, called the red-red zone, is well vascularized by branches from the geniculate arteries. Tears in this zone have the best healing potential because blood brings in nutrients and cells that promote tissue repair.
- Red-red = good vascular supply, good healing
- The middle one-third, or red-white zone, has only partial vascularity. Repairs here can heal, but success rates are lower than in the red-red zone.
- Red-white = limited vascularity, borderline healing
- The inner one-third, the white-white zone, is completely avascular and depends on diffusion from synovial fluid. Tears in this zone generally do not heal well, which is why repairs here often fail and partial meniscectomy is more commonly performed.
- White-white = no direct vascular supply, poor healing.
The blood supply to the meniscus comes primarily from the peripheral vascular plexus, which is fed by the
genicular arteries.
- Superior medial genicular artery
- Superior lateral genicular artery
- Inferior medial genicular artery
- Inferior lateral genicular artery
- Middle genicular artery
These arteries branch from the
popliteal artery, form a perimeniscal capillary plexus around the meniscal periphery, and send small radial branches into the meniscus.
- This explains why only the outer 10–30% (red-red zone) receives direct blood supply, while the inner zones rely on diffusion from synovial fluid.