Episode 4
Patellar Instability
Listen to Episode:
Objectives:
After listening to this episode, we hope that you can:
- Describe the typical presentation and mechanism of acute patellar dislocation and subluxation.
- Identify key anatomical and biomechanical risk factors contributing to instability.
- Explain the role of clinical exam maneuvers and imaging in diagnosis and preoperative planning.
- Compare non‑operative and operative management approaches, including indications and techniques.
- Outline a patient‑specific rehabilitation timeline and strategies to reduce recurrence risk.
Show Notes
Episode 4: Patellar Instability
Patellar instability often due to underlying anatomic factors that predispose the patella to maltracking and recurrent dislocation, particularly during activities that place valgus and rotational stress across the knee. Recognition of these contributors is essential, as they directly influence both clinical decision-making and surgical planning.
Key anatomic factors include patella alta, trochlear dysplasia, an increased tibial tubercle–trochlear groove (TT–TG) distance, lateral patellar tilt, and imbalance between the vastus medialis obliquus (VMO) and vastus lateralis. The presence and severity of these abnormalities help explain why some patients experience recurrent instability and guide the selection of appropriate non-operative or operative treatment strategies.
Anatomic Factors
TT-TG Distance
The TT-TG distance measures how far laterally the tibial tubercle (where the patellar tendon inserts on the tibia) is positioned relative to the center of the trochlear groove (where the patella normally tracks). It’s measured on CT or MRI. A normal TT-TG is typically <15 mm. This matters for patellar instability because if the tibial tubercle is positioned too far laterally, it creates a strong lateral pull on the patella, increasing the risk of dislocation or subluxation, especially during knee extension. It's a key factor when deciding whether a tibial tubercle osteotomy (surgical medialization) is needed.
Patella Alta
Patella alta refers to a high-riding patella that sits farther above the trochlea than normal. Because of this elevated position, the patella does not engage the groove early during knee flexion, leaving it more exposed and susceptible to lateral dislocation when the quadriceps contract. Patella baja is the opposite, with a low riding patella.
Measuring Patellar Height
Patellar height can be assessed using several radiographic ratios, each comparing the position of the patella relative to the knee joint.
- The Insall–Salvati ratio compares patellar tendon length to patellar length (normal ~1.0; >1.2 = alta, <0.8 = baja). It must be measured in 30 degrees off flexion on a lateral XR.
- The Modified Insall–Salvati ratio adjusts for the position of the distal patellar articular surface relative to the tendon.
- The Blackburne–Peel ratio measures the distance from the tibial plateau to the lower pole of the patellar articular surface divided by articular length (normal ~0.8; >1.0 = alta, <0.5 = baja).
- The Caton–Deschamps index compares the distance from the tibial plateau to the inferior patellar articular surface to the length of the articular surface (normal ~1.0; >1.2 = alta, <0.6 = baja).
Each method has slightly different landmarks but all help diagnose patella alta (high-riding) or patella baja (low-riding).
Trochlear Dysplasia
Trochlear dysplasia is a condition where the trochlear groove—where the patella is supposed to glide—is shallow or flat instead of concave. This means the patella has less bony containment, making it easier for it to slip laterally during movement. Sometimes surgeons may do a trochleaplasty.
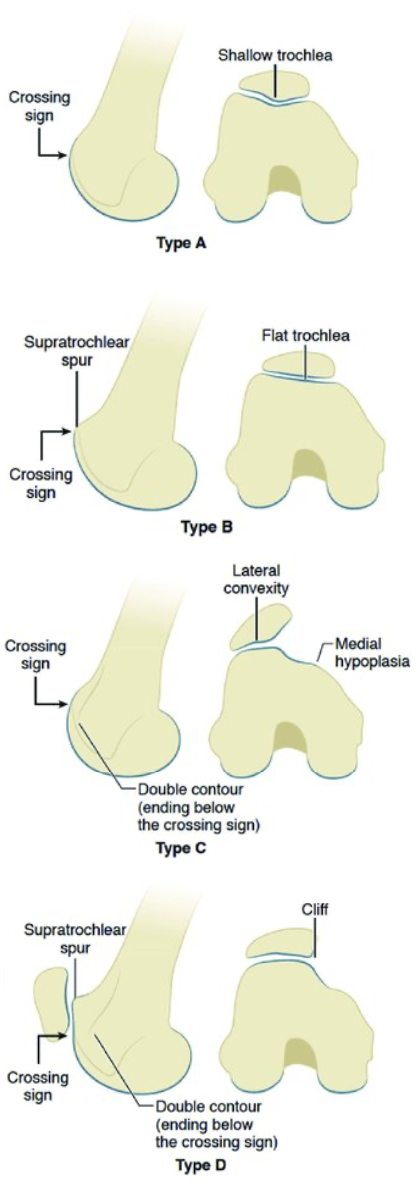
The DeJour classification is most used to classify trochlear dysplasia.
Type A:
Shallow but still concave trochlear groove with a crossing sign. Represents mild dysplasia and the lowest risk of instability.
Type B:
Flat or convex trochlea with a crossing sign and supratrochlear spur. Indicates moderate dysplasia with increased instability risk.
Type C:
Asymmetric trochlea with a hypoplastic medial facet and prominent lateral facet, showing a crossing sign and double contour. Associated with significant patellar maltracking.
Type D:
Severe “cliff-type” trochlea with crossing sign, supratrochlear spur, and double contour. Represents severe dysplasia and often requires bony correction.
Soft-Tissue Considerations
1) Lateral Patellar Tilt
Lateral patellar tilt means the patella is rotated so that its outer edge is elevated or angled outward. This tilt often reflects tightness in the lateral retinaculum or imbalance in soft tissues and makes the patella more likely to shift laterally instead of staying centered.
2) VMO Imbalance
Vastus lateralis imbalance refers to unequal strength or timing between the medial stabilizer of the patella (the vastus medialis oblique) and the more powerful lateral puller (vastus lateralis). If the VMO is weak or activates too late, the
stronger lateral forces dominate, pulling the patella outward and predisposing to instability. Initially physiotherapy during conservative management will target the VMO.